Free Quiz EBS
Quiz-summary
0 of 10 questions completed
Questions:
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
Information
This is a free quiz if you score 100% You Will Get Free 1 Hour Full Membership to Access Quiz
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
-
Congrats you have won a Free 1 Hour Full access membership.
Click here and Use coupon 1S2GEE to checkout for free.Please check your email for correct answers and explanations -
Please check your email for correct answers and explanations
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- Answered
- Review
-
Question 1 of 10
1. Question
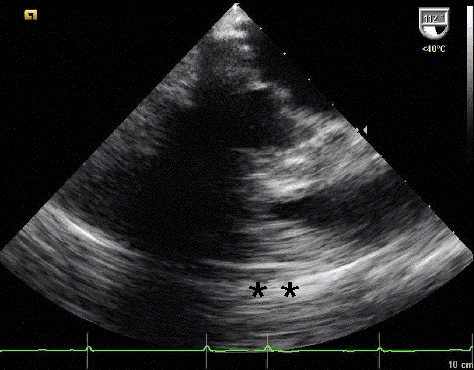
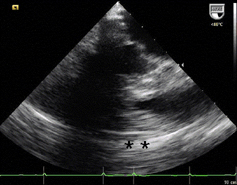
1 pointsA 76-year- old female undergoes transesophageal echocardiography (TEE) in preparation for direct current cardioversion. The following image is obtained at in the esophageal view at approximately 60 degrees. The black signal void moving across the heart throughout the cardiac cycle located to the left of the asterisks (**) is due to
 Correct
Correct
1). C
The shadow type of artifact seen in the TEE image represents attenuation of the ultrasound energy due to dense accumulation of calcific material along the mitral valve annular ring, also known as heavy mitral annular calcification. The key to this question is recognizing the imaging finding. It is similar to shadowing noted on abdominal ultrasound images of a gallstone within a gall bladder.Incorrect
1). C
The shadow type of artifact seen in the TEE image represents attenuation of the ultrasound energy due to dense accumulation of calcific material along the mitral valve annular ring, also known as heavy mitral annular calcification. The key to this question is recognizing the imaging finding. It is similar to shadowing noted on abdominal ultrasound images of a gallstone within a gall bladder. -
Question 2 of 10
2. Question
1 pointsWhat echocardiographic view is shown below?
 Correct
Correct
2). E
The view shown is a transthoracic subcostal short axis view of the right atrium, interatrial septum, aortic valve, right ventricle, and the left atrium. Nodular sclerosis of the non-coronary aortic valve cusp and an aneurismal interatrial septum are noted. Students of echocardiography should realize that much practice is needed to instantly recognize the views in cardiac ultrasound. Students are strongly encouraged to read frequently and practice with their peers and teachers to gain confidence in this regard. Often, recognizable clues in the image help to determine which view has been obtained. If liver tissue is present on the left side of the screen, subcostal transthoracic is likely; in this case, liver, inferior vena cava, and portions of hepatic veins are present, suggesting this possibility. If the ventricular apex is at the bottom of the screen and the image appears particularly clear, transesophageal views are likely. Transesophageal views from a deep transgastric orientation can often be recognized by liver tissue at the left of the screen, similar to subcostal views. Occasionally, the image may show a transducer angle in the upper right portion of the imaging, confirming that the image that was acquired is a transesophageal echocardiogram.
Importantly, all views in echocardiography are approximations and by their very nature are taken on a double oblique axis; practice with an expert in the field is needed to quickly recognize and discern complex echocardiograms. Facility with different views and “how normal should appear” is needed to then determine how to look for cardiac pathology.Incorrect
2). E
The view shown is a transthoracic subcostal short axis view of the right atrium, interatrial septum, aortic valve, right ventricle, and the left atrium. Nodular sclerosis of the non-coronary aortic valve cusp and an aneurismal interatrial septum are noted. Students of echocardiography should realize that much practice is needed to instantly recognize the views in cardiac ultrasound. Students are strongly encouraged to read frequently and practice with their peers and teachers to gain confidence in this regard. Often, recognizable clues in the image help to determine which view has been obtained. If liver tissue is present on the left side of the screen, subcostal transthoracic is likely; in this case, liver, inferior vena cava, and portions of hepatic veins are present, suggesting this possibility. If the ventricular apex is at the bottom of the screen and the image appears particularly clear, transesophageal views are likely. Transesophageal views from a deep transgastric orientation can often be recognized by liver tissue at the left of the screen, similar to subcostal views. Occasionally, the image may show a transducer angle in the upper right portion of the imaging, confirming that the image that was acquired is a transesophageal echocardiogram.
Importantly, all views in echocardiography are approximations and by their very nature are taken on a double oblique axis; practice with an expert in the field is needed to quickly recognize and discern complex echocardiograms. Facility with different views and “how normal should appear” is needed to then determine how to look for cardiac pathology. -
Question 3 of 10
3. Question
1 pointsA continuous wave echocardiogram is obtained across a regurgitant pulmonic valve. In early diastole, the peak regurgitant velocity by Doppler is 2.9 cm/sec and the, at end diastole, the regurgitant velocity is 1.5 m/sec, across the pulmonic valve. What is the approximate pulmonary capillary wedge pressure assuming a right atrial pressure of 8 mm Hg and no tricuspid stenosis?
Correct
3). B
The tracing reveals a diastolic jet with a peak velocity of about 2.9 m/sec and an end diastolic velocity of about 1.5 m/sec. At end-diastole, pulmonary artery pressure is approximately equal to left atrial (or pulmonary capillary wedge) pressure. Also at diastole, right atrial and ventricular pressures are approximately equal. Using the Bernoulli principle, the gradient across the pulmonic valve (∆P) is given by ∆P = 4 *(1.5)2, which equals approximately 9 mm Hg. Since, at end diastole, pulmonary artery pressure equals right ventricular pressure equals right atrial pressure (if there is no tricuspid stenosis, as specified in the question), adding this gradient to right atrial pressure yields a useful estimate of pulmonary artery diastolic pressure, which is approximately equal to left atrial pressure, by echocardiography.
Incorrect
3). B
The tracing reveals a diastolic jet with a peak velocity of about 2.9 m/sec and an end diastolic velocity of about 1.5 m/sec. At end-diastole, pulmonary artery pressure is approximately equal to left atrial (or pulmonary capillary wedge) pressure. Also at diastole, right atrial and ventricular pressures are approximately equal. Using the Bernoulli principle, the gradient across the pulmonic valve (∆P) is given by ∆P = 4 *(1.5)2, which equals approximately 9 mm Hg. Since, at end diastole, pulmonary artery pressure equals right ventricular pressure equals right atrial pressure (if there is no tricuspid stenosis, as specified in the question), adding this gradient to right atrial pressure yields a useful estimate of pulmonary artery diastolic pressure, which is approximately equal to left atrial pressure, by echocardiography.
-
Question 4 of 10
4. Question
1 pointsThe echocardiogram shown is obtained in a patient who is status post mechanical aortic valve surgery. The small moving objects below the valve and inside the left ventricular chamber represent
 Correct
Correct
4). D
Cavitation occurs due to significant local pressure variations created by the fast movement of flat, stiff surfaces on prosthetic valves. Local acceleration of blood over hinge point creates a pressure gradient that, when high enough, can cause spontaneous gas formation from the surface below, referred to as the cavitation phenomenon. Specifically, when the pressure gradient created by fast moving mechanical mitral valve surfaces exceeds vapor pressure of the blood itself, micro bubbles form. The cavitation phenomenon revealed in this echocardiogram is seen in more familiar examples, such as with a boat propeller that is completely underwater. When the rotational velocity is high enough, bubbles are formed at the interface of the water and the propeller surface and are visible above the running propeller. The finding on routine echocardiography can be a normal postoperative variant or can imply mechanical failure in part of the prosthetic valve. In general, valve configurations and/or hemodynamics that minimize cavitation tend to reduce hemolysis due to mechanical valves.
Incorrect
4). D
Cavitation occurs due to significant local pressure variations created by the fast movement of flat, stiff surfaces on prosthetic valves. Local acceleration of blood over hinge point creates a pressure gradient that, when high enough, can cause spontaneous gas formation from the surface below, referred to as the cavitation phenomenon. Specifically, when the pressure gradient created by fast moving mechanical mitral valve surfaces exceeds vapor pressure of the blood itself, micro bubbles form. The cavitation phenomenon revealed in this echocardiogram is seen in more familiar examples, such as with a boat propeller that is completely underwater. When the rotational velocity is high enough, bubbles are formed at the interface of the water and the propeller surface and are visible above the running propeller. The finding on routine echocardiography can be a normal postoperative variant or can imply mechanical failure in part of the prosthetic valve. In general, valve configurations and/or hemodynamics that minimize cavitation tend to reduce hemolysis due to mechanical valves.
-
Question 5 of 10
5. Question
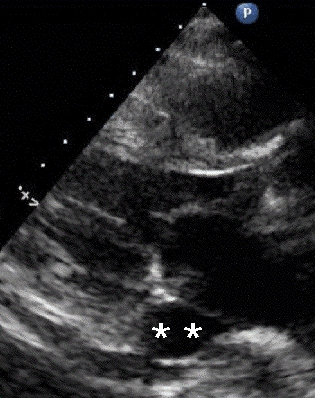
1 pointsA 36-year- old female patient complains of shortness of breath. The following parasternal long axis image is obtained. The most likely anatomical variant in the thorax that is associated with this particular echocardiographic finding indicated by the asterisks (**) is:

 Correct
Correct
5). C
The structure depicted is a dilated coronary sinus (CS), most likely due to an aberrant left sided superior vena cava (SVC) that drains directions to the CS rather than to the right atrium. This is usually asymptomatic and does not require further treatment or follow up. The presence of a dilated CS due to a left sided SVC can be confirmed by injecting agitated saline into a left arm intravenous catheter and monitoring transit in a suitable view; normally, agitated saline arrives first in the right atrium; in patients with a left sided SVC draining directly to the CS, contrast will arrive first in the CS, then right atrium, then RV. In the parasternal long axis view shown, contrast would be expected to arrive in the right ventricle before the CS in normal circulation. A coronary arteriovenous fistula can cause dilatation of the coronary veins, including the middle cardiac vein (MCV). This particular view is not usually helpful for visualizing this portion of the cardiac venous anatomy. Biventricular pacemaker implantation has been described in such patients and, while challenging to most implanters, is feasible usually with caution due to need to navigate antegrade (rather than retrograde) through the coronary sinus.
Incorrect
5). C
The structure depicted is a dilated coronary sinus (CS), most likely due to an aberrant left sided superior vena cava (SVC) that drains directions to the CS rather than to the right atrium. This is usually asymptomatic and does not require further treatment or follow up. The presence of a dilated CS due to a left sided SVC can be confirmed by injecting agitated saline into a left arm intravenous catheter and monitoring transit in a suitable view; normally, agitated saline arrives first in the right atrium; in patients with a left sided SVC draining directly to the CS, contrast will arrive first in the CS, then right atrium, then RV. In the parasternal long axis view shown, contrast would be expected to arrive in the right ventricle before the CS in normal circulation. A coronary arteriovenous fistula can cause dilatation of the coronary veins, including the middle cardiac vein (MCV). This particular view is not usually helpful for visualizing this portion of the cardiac venous anatomy. Biventricular pacemaker implantation has been described in such patients and, while challenging to most implanters, is feasible usually with caution due to need to navigate antegrade (rather than retrograde) through the coronary sinus.
-
Question 6 of 10
6. Question
1 pointsA 41 year-old- female is evaluated by echocardiography for a murmur. Cor triatriatum sinister is found. This finding is most commonly associated with what other congenital defect?
Correct
6). C
Cor triatriatum sinister refers to a congenital cardiac condition whereby primitive septation remnants in the left atrium divide the chamber into three communicating portions. When this finding occurs in the right atrium, it is referred to as cor triatriatum dexter. Cor triatriatum sinister is associated with anomalous pulmonary venous return, which can be identified by a carefully performed transesophageal echocardiography (TEE), contrast computed tomography (CT) or magnetic resonance imaging (MRI) with appropriate bolus timing. Anomalous pulmonary venous return can also be identified intra operatively, as dictated by the clinical situation.
Incorrect
6). C
Cor triatriatum sinister refers to a congenital cardiac condition whereby primitive septation remnants in the left atrium divide the chamber into three communicating portions. When this finding occurs in the right atrium, it is referred to as cor triatriatum dexter. Cor triatriatum sinister is associated with anomalous pulmonary venous return, which can be identified by a carefully performed transesophageal echocardiography (TEE), contrast computed tomography (CT) or magnetic resonance imaging (MRI) with appropriate bolus timing. Anomalous pulmonary venous return can also be identified intra operatively, as dictated by the clinical situation.
-
Question 7 of 10
7. Question
1 pointsThe speed of sound in myocardium is approximately
Correct
7). C
Speed of sound in tissues (including heart) is approximately 1540 m/sec. The focus of this question is the correct units.
Incorrect
7). C
Speed of sound in tissues (including heart) is approximately 1540 m/sec. The focus of this question is the correct units.
-
Question 8 of 10
8. Question
1 pointsThe reduction in pressure seen in the left ventricular outflow tract (LVOT) during mechanical systole in a patient with hyperdynamic contraction of the basal myocardium resulting in reduction in the LVOT size and increase in the velocity across the LVOT is described by which physics principle?
Correct
8). D
The Venturi effect describes the relative reduction in pressure – a partial vacuum – that occurs when fast moving viscous fluids traverse across a flat surface. For patients with dynamic left ventricular outflow tract (LVOT) obstruction where there is fast moving blood present above the mitral valve leaflets, this produces a lower pressure across the ventricular surface of the mitral valve, which can cause abnormal systolic anterior motion (SAM) of the mitral valve and mitral regurgitation in such patients. The mitral regurgitation due to SAM in the presence of significant left ventricular hypertrophy is referred to as hypertrophic obstructive cardiomyopathy (HOCM) physiology; it should be noted that HOCM physiology does not necessarily indicate the actual disease state of HOCM.
Incorrect
8). D
The Venturi effect describes the relative reduction in pressure – a partial vacuum – that occurs when fast moving viscous fluids traverse across a flat surface. For patients with dynamic left ventricular outflow tract (LVOT) obstruction where there is fast moving blood present above the mitral valve leaflets, this produces a lower pressure across the ventricular surface of the mitral valve, which can cause abnormal systolic anterior motion (SAM) of the mitral valve and mitral regurgitation in such patients. The mitral regurgitation due to SAM in the presence of significant left ventricular hypertrophy is referred to as hypertrophic obstructive cardiomyopathy (HOCM) physiology; it should be noted that HOCM physiology does not necessarily indicate the actual disease state of HOCM.
-
Question 9 of 10
9. Question
1 pointsWhich ultrasound frequency range is most suitable for typical adult echocardiography?
Correct
9). D
Typical adult echocardiography is done with ultrasound frequency in the two to three Megahertz range. In general, higher frequency sound waves have less penetration, whereas lower frequency waves provide more penetration.
Incorrect
9). D
Typical adult echocardiography is done with ultrasound frequency in the two to three Megahertz range. In general, higher frequency sound waves have less penetration, whereas lower frequency waves provide more penetration.
-
Question 10 of 10
10. Question
1 pointsEchocardiogram is requested on a 39-year- old male with moderate emphysema who weighs 327 pounds. Images are suboptimal. Intravenous contrast is given after appropriate agitation and dilution. After allowing a time for blood level equilibration, how should the instrument be adjusted to optimize imaging?
Correct
10). D
In general, reducing the mechanical index after administration of ventricular contrast agitated microbubbles provides optimal echocardiographic appearance. Contrast administration can be considered in patients who are obese, have barrel chests due to lung disease, and/or who have poor imaging windows based on anatomy.
Incorrect
10). D
In general, reducing the mechanical index after administration of ventricular contrast agitated microbubbles provides optimal echocardiographic appearance. Contrast administration can be considered in patients who are obese, have barrel chests due to lung disease, and/or who have poor imaging windows based on anatomy.