Section-1
Quiz-summary
0 of 10 questions completed
Questions:
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
Information
Click to begin Section-1 Quiz
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- Answered
- Review
-
Question 1 of 10
1. Question
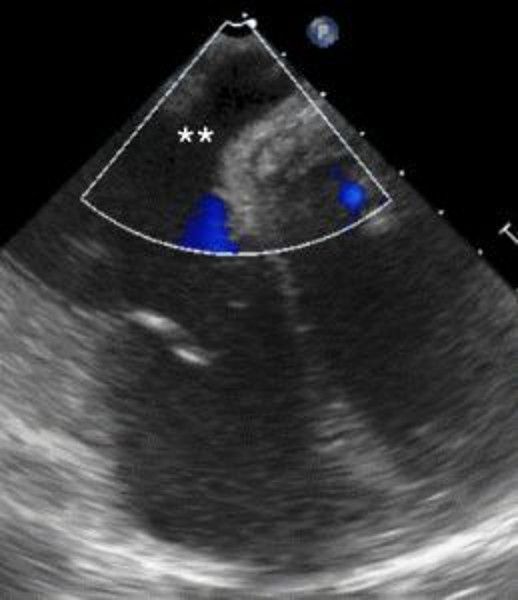
1 pointsThe following transesophageal echo image is obtained after passing the probe to the gastro-esophageal junction at 0 degrees with slight counter clockwise rotation. The area with Color Doppler flow indicated by the asterisks (**) is
 Correct
Correct
The structure depicted is the coronary sinus (CS), in normal anatomic position, posterior and basal in the heart, draining deoxygenated blood from the myocardium into the right atrium. The typical appearance of the tricuspid valve and interatrial septum are good landmarks in this image. This TEE view can be useful in assessing the position of the CS for operative cases where the CS is cannulated (e.g. during mitral valve repair), for biventricular pacing, and in evaluating patients with right to left shunts, among other things. This view is not always obtainable on TEE even when performed by experienced operators due to patient body habitus.
Incorrect
The structure depicted is the coronary sinus (CS), in normal anatomic position, posterior and basal in the heart, draining deoxygenated blood from the myocardium into the right atrium. The typical appearance of the tricuspid valve and interatrial septum are good landmarks in this image. This TEE view can be useful in assessing the position of the CS for operative cases where the CS is cannulated (e.g. during mitral valve repair), for biventricular pacing, and in evaluating patients with right to left shunts, among other things. This view is not always obtainable on TEE even when performed by experienced operators due to patient body habitus.
-
Question 2 of 10
2. Question
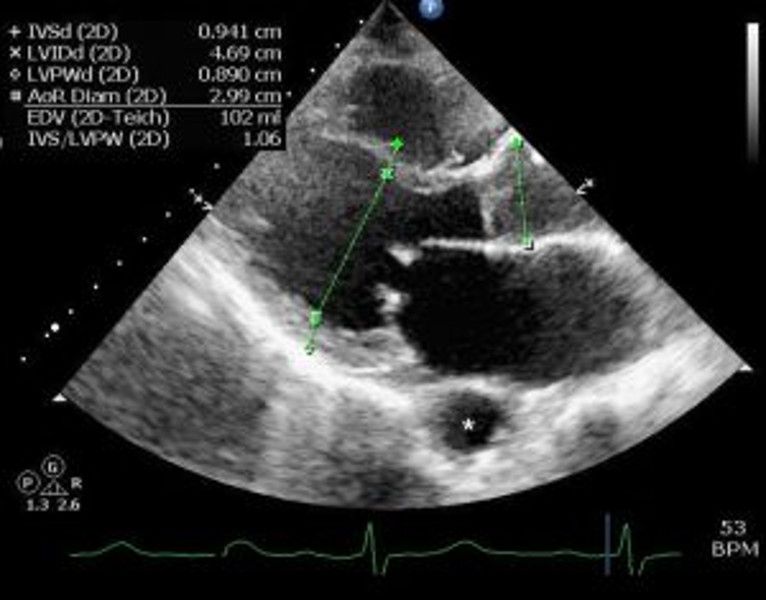
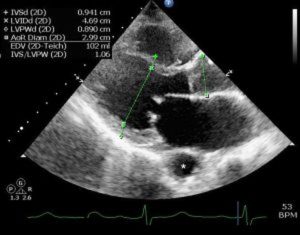
1 pointsA 42-year-old gentleman is evaluated for atypical chest pain. The following echocardiogram is obtained. Identify the structure denoted by the asterisk (*):
 Correct
Correct
The structure in the echocardiogram can be identified as descending thoracic aorta by ascertaining its relationship to the pericardium. The structure depicted is outside of the pericardium and most likely represents aorta. Other choices are less likely; the picture depicted is typical for the appearance of the thoracic aorta on parasternal long axis imaging. Were it within the pericardium, it would have been more likely to be a dilated coronary sinus.
Incorrect
The structure in the echocardiogram can be identified as descending thoracic aorta by ascertaining its relationship to the pericardium. The structure depicted is outside of the pericardium and most likely represents aorta. Other choices are less likely; the picture depicted is typical for the appearance of the thoracic aorta on parasternal long axis imaging. Were it within the pericardium, it would have been more likely to be a dilated coronary sinus.
-
Question 3 of 10
3. Question
1 pointsA 41 year-old-female is evaluated by echocardiography for a murmur. Cor triatriatum sinister is found. This finding is most commonly associated with what other congenital defect?
Correct
Cor triatriatum sinister refers to a congenital cardiac condition whereby primitive septation remnants in the left atrium divide the chamber into three communicating portions. When this finding occurs in the right atrium, it is referred to as cor triatriatum dexter. Cor triatriatum sinister is associated with anomalous pulmonary venous return, which can be identified by a carefully performed transesophageal echocardiography (TEE), contrast computed tomography (CT) or magnetic resonance imaging (MRI) with appropriate bolus timing. Anomalous pulmonary venous return can also be identified intra operatively, as dictated by the clinical situation.
Incorrect
Cor triatriatum sinister refers to a congenital cardiac condition whereby primitive septation remnants in the left atrium divide the chamber into three communicating portions. When this finding occurs in the right atrium, it is referred to as cor triatriatum dexter. Cor triatriatum sinister is associated with anomalous pulmonary venous return, which can be identified by a carefully performed transesophageal echocardiography (TEE), contrast computed tomography (CT) or magnetic resonance imaging (MRI) with appropriate bolus timing. Anomalous pulmonary venous return can also be identified intra operatively, as dictated by the clinical situation.
-
Question 4 of 10
4. Question
1 pointsA 36-year-old female with complaints of severe episodic palpitations, labile hypertension between 140/90 to 220/110 mm Hg, sweating, exertional shortness of breath, and feeling of exhaustion. Transthoracic echo reveals mild concentric ventricular hypertrophy and a markedly hyperdynamic heart. Urine and serum cathecholamines are elevated. CT scan of the abdomen reveals normal adrenal glands and a 4 cm “para aortic body” near the inferior mesenteric artery. A pheochromocytoma is suspected.
The likely cause of hyperdynamic ventricular function and labile hypertension is enlargement and abnormal epinephrine secretion from the
Correct
A common location of abnormal catecholamine secreting tumors outside of the adrenal glands is along the abdominal aorta itself, with enlargement of the Organ of Zuckerkandl, which is derived from neural crest cells, begins at the superior mesenteric artery and extends to the iliac bifurcation, and is usually composed of a mass of chromaffin cells. Early in development, it is involved with homeostatic regulation of blood pressure; later, it normally regresses and becomes the adult paraganglia. In patients with normal appearing adrenal glands and elevated catecholamine levels, abdominal imaging can be useful in looking for an enlarged Organ of Zuckerkandl, also known as a paraaortic body.
Incorrect
A common location of abnormal catecholamine secreting tumors outside of the adrenal glands is along the abdominal aorta itself, with enlargement of the Organ of Zuckerkandl, which is derived from neural crest cells, begins at the superior mesenteric artery and extends to the iliac bifurcation, and is usually composed of a mass of chromaffin cells. Early in development, it is involved with homeostatic regulation of blood pressure; later, it normally regresses and becomes the adult paraganglia. In patients with normal appearing adrenal glands and elevated catecholamine levels, abdominal imaging can be useful in looking for an enlarged Organ of Zuckerkandl, also known as a paraaortic body.
-
Question 5 of 10
5. Question
1 pointsA 37-year-old female with no significant prior past medical history complains of severe shortness of breath with exertion that has worsened recently. On exam, she has a decrescendo diastolic murmur with an opening snap 70 milliseconds after S2 best heard at the left sternal border. Echocardiography reveals severe mitral stenosis. Which of the following criteria are not incorporated into the Wilkins score to determine suitability for percutaneous balloon mitral valvuloplasty?
Correct
The four components of the Wilkins score to determine suitability for percutaneous balloon mitral valvuloplasty include degree of valvular calcification (score 0-4), chordal mobility (score 0-4), the nature of the subvalvular apparatus (score 0-4) and mitral leaflet thickness (score 0-4). Added up, the score is 0-16. A score of 8 or higher for a particular patient implies percutaneous balloon mitral valvuloplasty may not produce favorable results.
Incorrect
The four components of the Wilkins score to determine suitability for percutaneous balloon mitral valvuloplasty include degree of valvular calcification (score 0-4), chordal mobility (score 0-4), the nature of the subvalvular apparatus (score 0-4) and mitral leaflet thickness (score 0-4). Added up, the score is 0-16. A score of 8 or higher for a particular patient implies percutaneous balloon mitral valvuloplasty may not produce favorable results.
-
Question 6 of 10
6. Question
1 pointsA 37-year-old female with no significant prior past medical history complains of severe shortness of breath with exertion that has worsened recently. On exam, she has a decrescendo diastolic murmur with an opening snap 70 milliseconds after S2 best heard at the left sternal border. Echocardiography reveals severe mitral stenosis. A subtle systolic murmur radiating to the axilla is also appreciated. Echocardiography confirms mitral regurgitation. Which of these is a contraindication to percutaneous balloon mitral valvuloplasty?
Correct
Although not at all intuitive, mild and moderate mitral regurgitation are not contraindications to percutaneous balloon mitral valvuloplasty. Percutaneous commissurotomy and valvuloplasty does not alter the degree of mitral regurgitation in most patients undergoing the procedure. It is thought that coaptation remains unchanged despite high-pressure large-bore balloon inflation across the valve. Severe mitral regurgitation does represent a contraindication to percutaneous balloon mitral valvuloplasty because the degree of regurgitation by itself constitutes an indication for valve surgery and does not improve post valvuloplasty. The finding of thickened mitral leaflets by itself only represents one of four Wilkins criteria for percutaneous balloon mitral valvuloplasty and is not in and of itself a contraindication.
Incorrect
Although not at all intuitive, mild and moderate mitral regurgitation are not contraindications to percutaneous balloon mitral valvuloplasty. Percutaneous commissurotomy and valvuloplasty does not alter the degree of mitral regurgitation in most patients undergoing the procedure. It is thought that coaptation remains unchanged despite high-pressure large-bore balloon inflation across the valve. Severe mitral regurgitation does represent a contraindication to percutaneous balloon mitral valvuloplasty because the degree of regurgitation by itself constitutes an indication for valve surgery and does not improve post valvuloplasty. The finding of thickened mitral leaflets by itself only represents one of four Wilkins criteria for percutaneous balloon mitral valvuloplasty and is not in and of itself a contraindication.
-
Question 7 of 10
7. Question
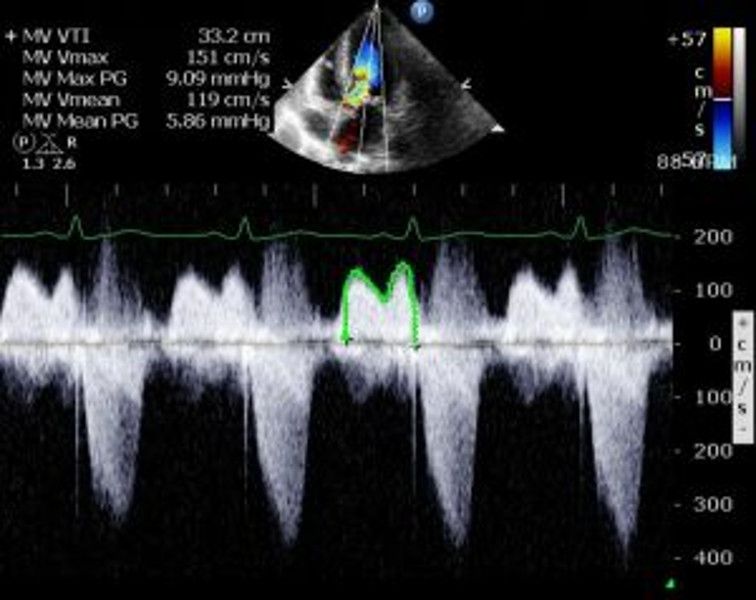
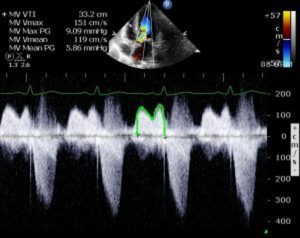
1 pointsWhat is the diagnosis that can be inferred from echocardiogram shown below in a patient with a left atrial myxoma?
 Correct
Correct
This is a classic continuous wave (CW) Doppler image through the mitral valve in a patient with a left atrial (LA) myxoma revealing mitral stenosis. LA myxoma causes mitral stenosis physiology via an anatomic obstruction into the LV chamber from the left atrium. LA myxoma is most clinically apparent when it mimics significant mitral stenosis, and at least mild mitral stenosis is suggested by the CW waveform shown. Next clinical step for management of a patient with this finding would probably be referral for excision of the tumor, which usually includes separate preoperative coronary angiography and TEE evaluation.
Incorrect
This is a classic continuous wave (CW) Doppler image through the mitral valve in a patient with a left atrial (LA) myxoma revealing mitral stenosis. LA myxoma causes mitral stenosis physiology via an anatomic obstruction into the LV chamber from the left atrium. LA myxoma is most clinically apparent when it mimics significant mitral stenosis, and at least mild mitral stenosis is suggested by the CW waveform shown. Next clinical step for management of a patient with this finding would probably be referral for excision of the tumor, which usually includes separate preoperative coronary angiography and TEE evaluation.
-
Question 8 of 10
8. Question
1 pointsMeasurement of the left atrial dimension is most accurate in which view:
Correct
A non-foreshortened apical four-chamber view allows for the most standardized, reproducible, accurate measurement of the left atrial size on 2D TTE.
In general, sizes are measured on the parasternal views as well and are useful; however, the variable nature of this view can cause over or underestimation of the true size. Recent studies indicate that, in fact, calculation of left atrial areas and volumes may be superior to 2D measurements as they help to cover more regions of the left atrial chamber. Nonetheless, left atrial dimensions are still routinely measured and reported. The apical four-chamber view is best for this purpose.
Incorrect
A non-foreshortened apical four-chamber view allows for the most standardized, reproducible, accurate measurement of the left atrial size on 2D TTE.
In general, sizes are measured on the parasternal views as well and are useful; however, the variable nature of this view can cause over or underestimation of the true size. Recent studies indicate that, in fact, calculation of left atrial areas and volumes may be superior to 2D measurements as they help to cover more regions of the left atrial chamber. Nonetheless, left atrial dimensions are still routinely measured and reported. The apical four-chamber view is best for this purpose.
-
Question 9 of 10
9. Question
1 pointsWhich leaflet of the tricuspid valve is most frequently downwardly displaced in Ebstein’s Anomaly?
Correct
Ebstein’s anomaly is a congenital downward displacement of one or more tricuspid valve leaflets, frequently the septal and posterior leaflets. It is usually associated with tricuspid regurgitation and can be corrected surgically with Carpentier or Danielson repair techniques.
The tricuspid valve consists of three leaflets: anterior, septal, and posterior.
Incorrect
Ebstein’s anomaly is a congenital downward displacement of one or more tricuspid valve leaflets, frequently the septal and posterior leaflets. It is usually associated with tricuspid regurgitation and can be corrected surgically with Carpentier or Danielson repair techniques.
The tricuspid valve consists of three leaflets: anterior, septal, and posterior.
-
Question 10 of 10
10. Question
1 pointsWhat is the most reliable measurement to diagnose or to rule out cardiac tamponade?
Correct
Cardiac tamponade can be diagnosed several ways and all the measurements noted can be useful, depending on the clinical circumstance. The most reliable sonographic indicator of tamponade is inferior vena cava (IVC) dilatation with paradoxical increase in size with inspiration or sniff testing.
In general, external compression of the heart (i.e. tamponade) will first be manifest by increased driving force of venous blood flow to the heart, which is apparent clinically as distended neck veins with distant heart sounds, hemodynamically as increased central venous pressure and equalization of pressures in cardiac chambers, and echocardiographically as a dilated IVC and/or the failure of the IVC to collapse during sniff maneuver or deep inspiration (sonographic Kussmaul’s sign). This latter finding can be apparent either hemodynamically by examination of a central venous catheter waveform or sonographically by examining any large vein, and usually the IVC is the most easily visualized due to its size. In some cases (such as selective postoperative right atrial tamponade due to a clot), echo images of the heart are not obtainable due to ventilation, post-op state, or poor windows. In this case, the IVC size and/or central venous pressure may be the only reliable indicator of tamponade.
Incorrect
Cardiac tamponade can be diagnosed several ways and all the measurements noted can be useful, depending on the clinical circumstance. The most reliable sonographic indicator of tamponade is inferior vena cava (IVC) dilatation with paradoxical increase in size with inspiration or sniff testing.
In general, external compression of the heart (i.e. tamponade) will first be manifest by increased driving force of venous blood flow to the heart, which is apparent clinically as distended neck veins with distant heart sounds, hemodynamically as increased central venous pressure and equalization of pressures in cardiac chambers, and echocardiographically as a dilated IVC and/or the failure of the IVC to collapse during sniff maneuver or deep inspiration (sonographic Kussmaul’s sign). This latter finding can be apparent either hemodynamically by examination of a central venous catheter waveform or sonographically by examining any large vein, and usually the IVC is the most easily visualized due to its size. In some cases (such as selective postoperative right atrial tamponade due to a clot), echo images of the heart are not obtainable due to ventilation, post-op state, or poor windows. In this case, the IVC size and/or central venous pressure may be the only reliable indicator of tamponade.